
figure1
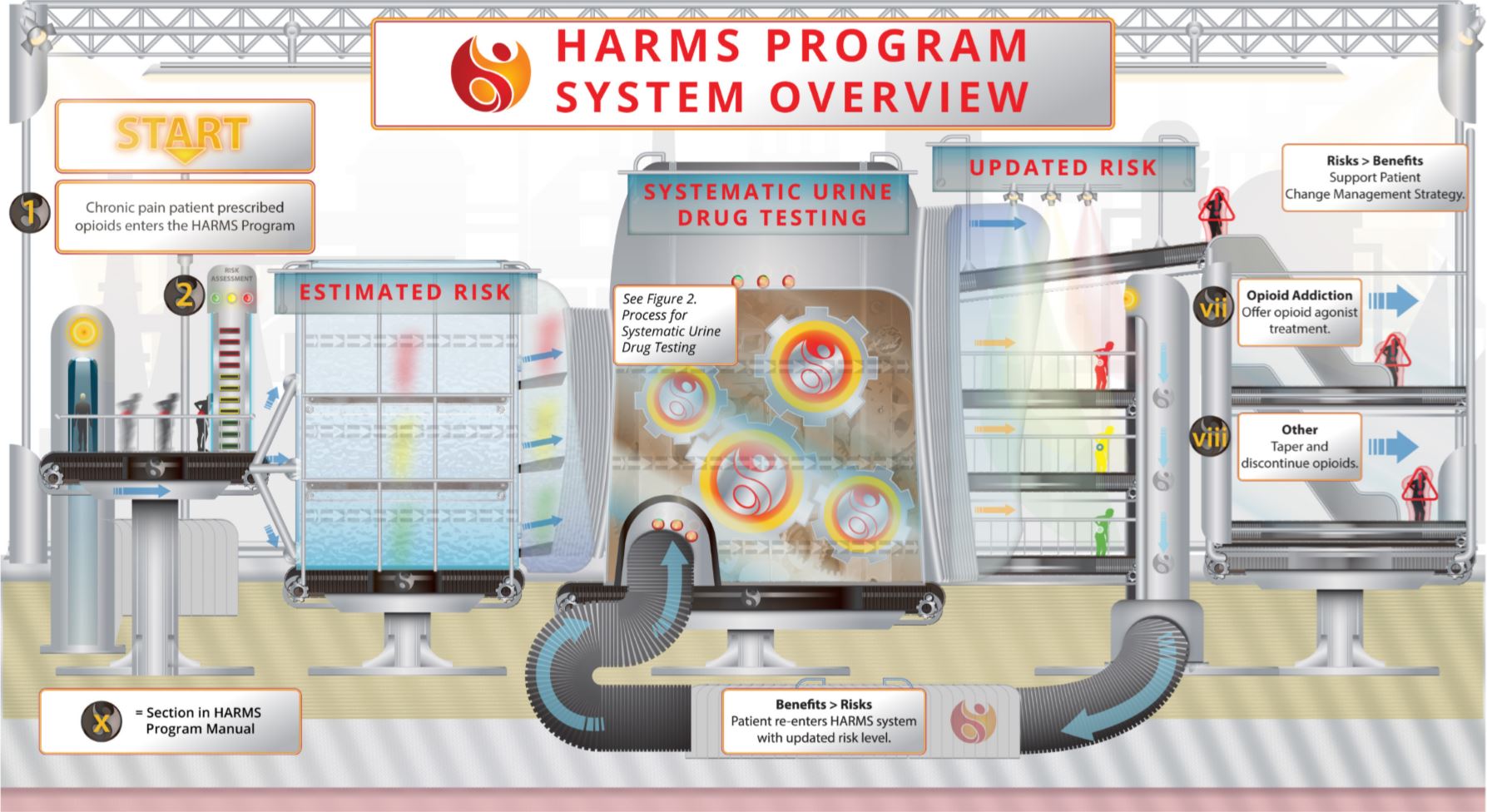
Illustrated here is an overview of the HARMS Program. Patients prescribed opioids for chronic non-cancer pain have their initial risk estimated based on any combination of validated risk stratification tool(s), past medical history, previous UDT results, behavioural observations, or simply the clinical Gestalt if physician time is a limiting factor for formalized stratification. The patient enters the UDT system (See Figure 2) with a risk estimate along a spectrum from low to high and UDT is conducted at a frequency concordant with that risk. As new information (from UDT or otherwise) tilts the risk/benefit balance, the risk is updated accordingly. If benefits still outweigh risks, then the patient re-enters the process using the updated risk level for the next iteration. Conversely, if it is found that risks outweigh benefits then the patient would be supported while management is changed. If opioids are no longer prescribed for chronic pain then that patient would exit the HARMS Program. It is critical when applying UDT to recognize that the intent is not to punish patients, but to inform the risk/benefit balance and guide subsequent patient discussion and management decisions.