
figure3
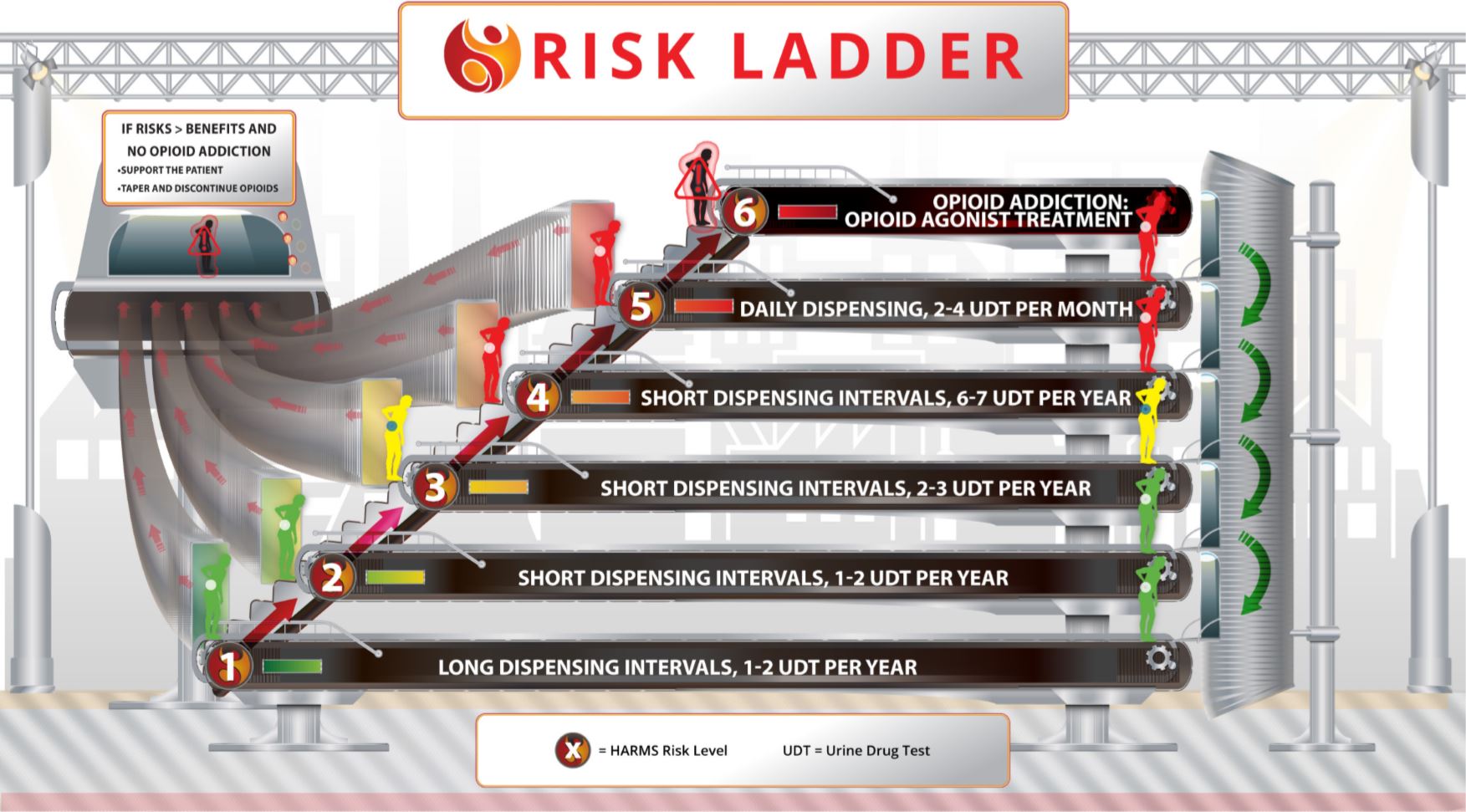
The Risk Ladder guides not only how to tailor prescribing and monitoring to a patient’s estimated risk, but it also advises how to move on the ladder in response to any situation. The initial risk estimate guides the starting place on the Risk Ladder, with subsequent movement on the ladder being informed by new information: UDT results, behavioural observations, mental health issues, changes in social stability, and any other new piece of information that informs the risk/benefit balance. The movement on the ladder is in direct proportion to the degree of concern. A significant concern (from UDT or otherwise) means significant movement up the ladder (as indicated by the red arrows). If opioid addiction is identified, then the patient moves to the top rung and opioid agonist treatment for addiction should be considered. Similarly, if the risks are greater than the benefits but there is no opioid addiction identified, then the patient moves off the ladder as support is given and management is changed. If the patient demonstrates clinical stability that lowers apparent risk and/or increases benefits, then he/she can move down the ladder (as indicated by the green arrows).