
Let’s describe these two different types of UDT in a little more detail, with specific, common examples illustrating key pearls.
IMMUNOASSAY
Basic science: this paragraph is not directly relevant to clinical practice and we would advise that you don’t need to know this, however we are also aware that some of you are curious about the basic science so have included it here. IA strips involve chromatography, antibodies and an agent that produces a signal we can detect. In the case of point-of-care IA, the signal that is produced is simply the presence or absence of a coloured strip to let us know if a certain drug or metabolite was in the sample tested. The urine will carry a chemically labelled antibody, by process of chromatography, across the test strip. The chemically labelled antibody will reach an area on the test strip coated with drug-protein conjugates and the antibody will bind to these conjugates. In the absence of any drug the antibodies will bind the conjugates, precipitate the chemical, and the label will become a detectable coloured line on the test strip showing a negative result (the second line). In the presence of drug the antibody sites will be occupied and no detectable line will form showing a positive drug result (a single line for the control).
Clinician’s Overview:
Now that some of the basic science is out of the way, let’s discuss a few caveats for IA. First of all, there is variability depending on the manufacturer (so not all “morphine” panels are created equal). Secondly, patients may tamper with their urine to either hide a drug that’s not supposed to be there, or add a drug they’re not taking that is supposed to be there (see Appendix III: Anti-tampering Techniques).
The test will generally result as “positive” or “negative”, however it very rarely may result as “invalid” (we’ve had one invalid result in 5 years) in which case it should be repeated immediately. The sensitivity and specificity for a panel, even for the same manufacturer, will have a natural variability depending on the dose and time the drug was taken, as well as individual variations in pharmacokinetics (absorption, distribution, metabolism and excretion). There are enormous lists of agents that have been reported to cause false positives for the IA various panels. Instead of covering these individually, we recommend you consult Moeller et al, 20175 or US Pharm. 20166 or if using START-IT then it will give you the more common causes of false positives for your specific results.
Now let’s go through scenarios and pearls when interpreting the most commonly used panels:
Morphine/Opiate Panel: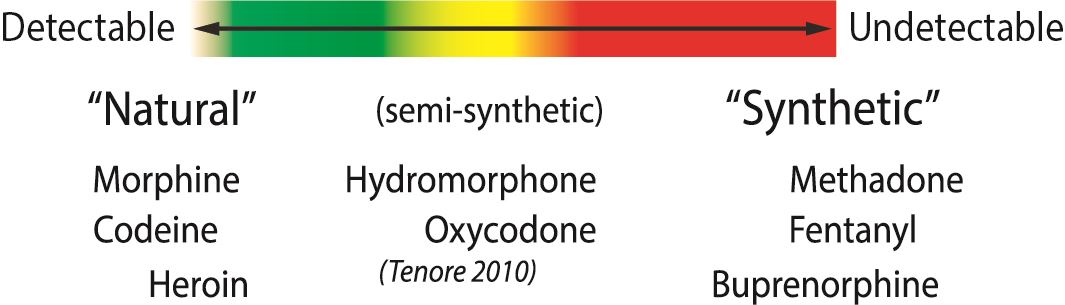
The morphine panel, also sometimes called the “opiate” panel (essentially the same thing), is very sensitive for detecting natural opioids. This includes codeine, morphine and (the mildly synthetic) heroin. The more synthetic an opioid, the less detectable. In fact, the fully synthetic opioids like fentanyl, methadone, tramadol and meperidine are not detectable on this panel. The semi-synthetics like oxycodone, hydromorphone and hydrocodone are variably detectable.
Practically, what this means is that if someone is prescribed hydromorphone for example, the morphine/opiate panel has limited utility. If the panel is positive, it suggests the person is taking hydromorphone (although it could be from another opioid). If the panel is negative, it doesn’t mean the person is not taking hydromorphone (high chance of false negative). If you are looking for a reliable test for the presence/ absence of the more synthetic opioids, then you should consider using specific panels for those drugs (they are commercially available for hydromorphone/hydrocodone, oxycodone, tramadol, methadone, fentanyl, and buprenorphine among others). Practically, you can start to go down the rabbit hole with number of panels so we use the 5 that we consider highest yield in our practice (Morphine, Oxycodone, EDDP (methadone), benzodiazepine and cocaine).
If the patient is prescribed morphine or codeine, then sensitivity of this panel is generally >90%. You will also note that this panel cannot distinguish between morphine/codeine/heroin. If relevant for your patient population, there is a specific IA panel for heroin which tests for a metabolite unique to heroin (6-MAM).
Oxycodone Panel:
The oxycodone panel unfortunately has a sensitivity that has been reported at 75%. This means that up to 25% of people who are actually taking their oxycodone may have a false negative. This of course is very important to know before accusing a patient of not taking his oxycodone just because the IA panel is negative.
Methadone (EDDP) Panel:
EDDP is the main metabolite of methadone. This is one of the most accurate IA panels with sensitivity of 96% and specificity of 99%.
Buprenorphine Panel:
Although studies have varied in the exact numbers, they all show the buprenorphine panel performs with high sensitivity (88-100%) and high specificity (87.5-100%). There have been reports of cross-reactivity with high concentrations of morphine, chloroquine and hydroxychloroquine.7-11
Benzodiazepine (BZD) Panel:
This is one of the more challenging panels because there is variability within the BZD class. In general, most BZD panels are designed to detect lipophilic BZD (oxazepam, temazepam, diazepam) and have a low sensitivity for clonazepam and lorazepam. However, even clonazepam and lorazepam are sometimes detected, so if a patient is prescribed lorazepam or clonazepam, this panel is generally not useful (a negative result cannot be acted on, a positive result supports that person took it but is not proof).
Cocaine Panel:
This is likely one of the most helpful panels when it’s positive. Specificity is reported as being as high as 100%12, so if cocaine IA panel is positive it means the person used cocaine. There are no agents known to cause false positives besides coca leaves. That said, sensitivity of this panel is low so it will frequently miss cocaine use.
Amphetamine Panel:
The amphetamine panel is the most difficult to interpret because of the many drugs that have cross-reactivities with this panel with many possibilities for false positives. Methamphetamine will likely be picked up by this panel but MDMA (ecstasy) is often missed and should be detected by an MDMA specific panel. Studies on the performance of amphetamine immunoassays vary greatly depending on the sample population they use because so many other drugs can cause false positives. In general this panel has been shown to have high sensitivities (around 100%) while the specificity can vary greatly (58-99%) depending on the patient population.13-16
Fentanyl Panel:
The fentanyl panel may be of increasing importance as more of it is found mixed into street drugs and for monitoring out-patients using fentanyl patches. There are fewer studies demonstrating the performance of fentanyl IA technologies but those that exist show high sensitivities (approx. 100%) and high specificities (86-99%). There has been report of cross reactivity with risperidone and trazodone. Fentanyl analogs like carfentanyl will also cause a cross-reaction but natural opioid analogues will not.17-19
Interpreting IA results:
To summarize, there is significant variability between the various IA panels in terms of sensitivity and specificity. Remember that results should be used to complement the rest of the clinical picture, and that with few exceptions IA can have false positives and negatives. First make sure that you know what the test result is suggesting, and if this suggestion is unexpected then consider explanations for a false positive/negative. Strongly consider confirmatory testing followed by an open discussion with the patient. It is very important that you understand the limitations of the test prior to discussing the results with the patient so as to not mismanage based on a misinterpretation or misunderstanding of the limitations of UDT. For more information about how to act on UDT (IA and/or LC-MS), see Chapter 9.
LIQUID CHROMATOGRAPHY-MASS SPECTROMETRY
Basic science: this paragraph is not directly relevant to clinical practice and we would advise that you don’t need to know this, however we are also aware that some of you are curious about the basic science so have included it here. Chromatography is the science of separating drugs, metabolites, proteins or other compounds based on their chemical properties. In chromatography you will always have a column with a stationary phase that is designed to retain these compounds in the column and a mobile phase that pushes the compounds out of the column. Based on chemical properties, every different compound will travel through the column at a different speed. In gas chromatography (GC) the stationary phase is a polymer and the mobile phase is a gas heated to extreme temperatures. The drugs or metabolites of interest must be also turned into a gas through extreme heat to be analyzed through gas chromatography. If it is not possible to become a gas the drug or metabolite will need to undertake a chemical derivatization reaction before entering the column. This increases the work to analyze your sample and limits the amount of substances that are possible to analyze. In liquid chromatography (LC) the sample is also placed on a column packed with a polymer but the mobile phase is pumped in at high pressures as a liquid solution. It is possible to analyze over 300 different substances at once using LC. The drugs or metabolites will be detected by a UV detector at the same time as their control would and can be accurately confirmed by tandem mass spectroscopy (MS) to identify the exact molecular weight of the substance leaving the column.20
LC-MS Clinician’s Overview:
Confirmatory testing is essential when the patient disagrees with the result suggested by presumptive testing (IA), or when you want to check for more drugs than are readily available on your IA panels. The LC-MS results include specific drugs and metabolites in the urine, and in theory should have a specificity of 100%. If a drug is detected, then the patient took it (or a parent drug). However, that said, we have had several examples of human error where a LC-MS report came back showing a drug was taken, but after adamant refusal by the patient and reinforcement from the rest of the clinical picture, the lab was contacted and there was a reporting error (i.e. the person didn’t actually have those drugs in their urine even though the report indicated that he did). The other time where you may get tricked, although not relevant in countries such as Canada where Vick’s Nasal inhaler is not available, is that Vick’s Nasal inhaler has methamphetamine, however it’s the enantiomer of the methamphetamine used in “speed” or crystal meth. The commonly used LC-MS cannot tell the difference. In other words, it might look like the person consumed “speed” when in fact it’s simply an over-the-counter nasal inhaler.
One of the more challenging aspects of interpreting LC-MS results is in knowing the numerous breakdown products. For example, codeine is metabolized into numerous other opioids and if you were not aware of this, you may see hydromorphone in someone’s urine who is prescribed codeine and falsely assume that he has been taking a non-prescribed opioid.
There are two ways to approach the vast amount of information when interpreting what a LC-MS result means. You could either start with the parent drug that the patient is supposed to be taking and look for the expected metabolite(s) to confirm consumption, or alternatively you could look at metabolites and work backwards to discern what this suggests about patient consumption. In general, it is easiest when looking at a prescribed drug to check for one of more metabolites. And when metabolite(s) show up that are not something you are expecting, you work backwards to determine what substance could cause this result.
One challenge that came up for us with several patients at our clinic revolved around impurities in prescribed medication. In an ideal world, a patient’s “morphine” medicine has 100% pure morphine, however unfortunately that’s not the case. As you can see from the table below, numerous opioids have impurities of closely related opioids. So if someone is on a high dose of one of these opioids, that could cause a “false positive” for another opioid on LC-MS.
Pearls for the more common LC-MS scenarios in clinical practice are described below:
Opiates (“natural” opioids like codeine/morphine and the mildly synthetic heroin):
Codeine is one of the most important opioids to know because it is the most commonly prescribed short-acting opioid in this province22 and it has so many metabolites that errors in interpretation are easy to make. As you can see below, codeine is broken down into morphine, hydromorphone and hydrocodone – all of whom are prescribable opioids (parent drugs) themselves. So if a patient has taken codeine, you cannot readily determine if he also ingested one of these other drugs. That said, if you see 6-MAM then this means that the person consumed heroin (it’s not part of codeine pathway). Another challenge is that poppy seeds actually contain very small amounts of codeine and morphine.23,24
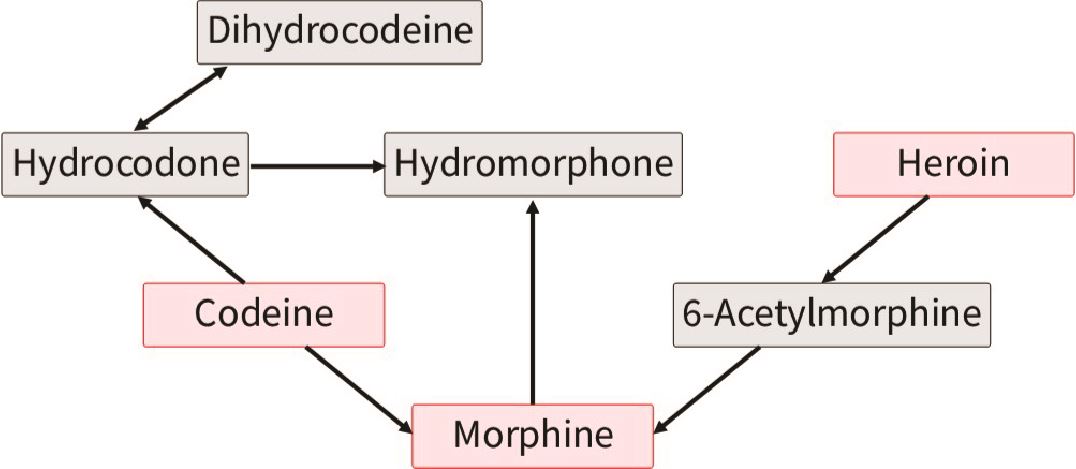
Figured adapted from Pesce et al. (2012)25
Likewise, you can see that if someone is taking morphine, then he may also have hydromorphone detected in his urine. While based on metabolism alone you would not expect someone prescribed hydromorphone to have morphine in his urine, or someone prescribed morphine to have codeine, remember from above that there can be impurities in the drug taken that are detectable (particularly at higher doses) and these do not necessarily indicate taking non-prescribed opioids.
Synthetic Opioids:
Contrasted to the opiates (“natural” opioids), the more synthetic opioids have their own metabolic pathways and are generally much simpler to interpret on LC-MS. Below are some examples of semi-synthetic and synthetic opioids, and what you may see on LC-MS:
- Oxycodone: Oxycodone, Oxymorphone, Noroxycodone
- Methadone: EDDP, Methadone
- Buprenorphine: Buprenorphine, Norbuprenorphine
- Tramadol: O-desmethyltramadol, N-Desmethyltramadol, tramadol
- Fentanyl: Norfentanyl, Fentanyl
 Figured adapted from Smolinska-Kempisty, et al. (2017)26
Figured adapted from Smolinska-Kempisty, et al. (2017)26
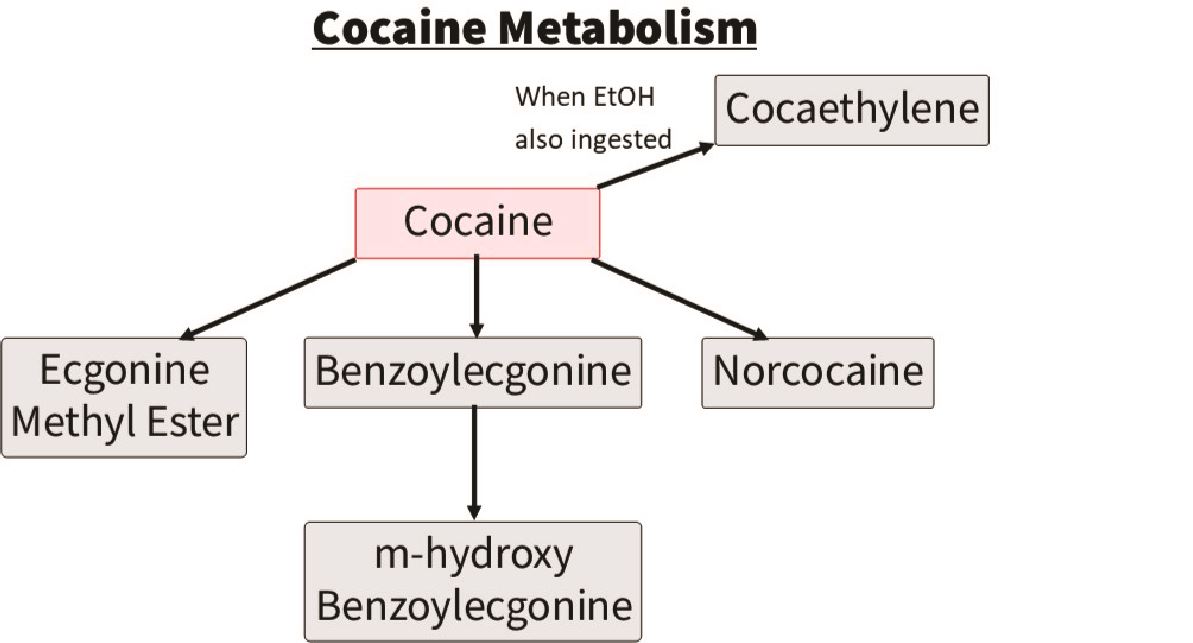
Cocaine:
The parent drug cocaine is rarely detected. The drug that is typically detected to indicate cocaine use is a metabolite of cocaine called benzoylecgonine. This stays in the urine ~3 days, however in heavy users can stay up to 10 days. The other drug commonly detected on LC-MS with cocaine use is levamisole, which is a cutting agent. You may also see cocaethylene which indicates alcohol and cocaine co-ingestion.
 Figured adapted from Pesce et al. (2012)25
Figured adapted from Pesce et al. (2012)25
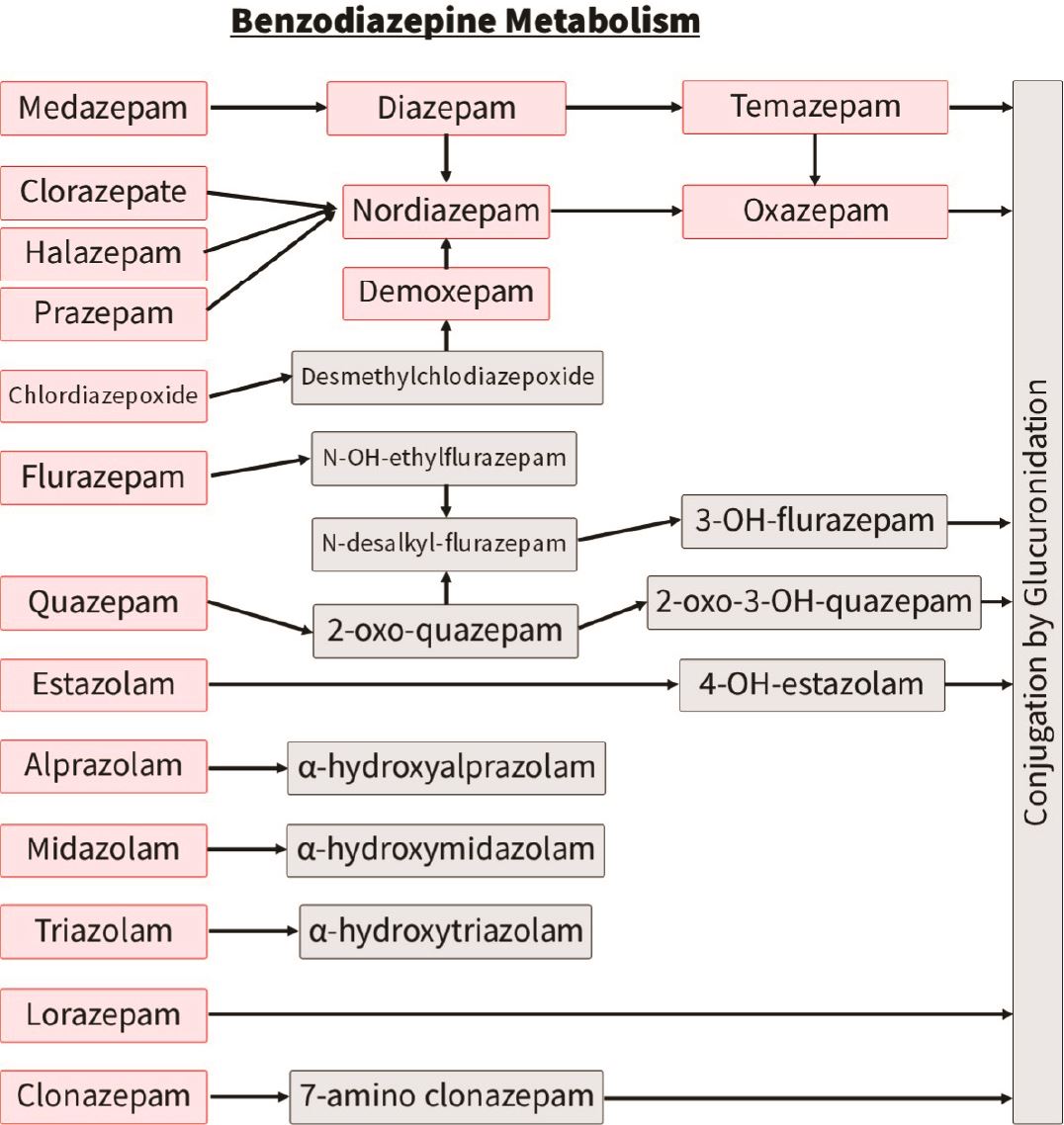
Benzodiazepines:
The most challenging benzodiazepines to interpret are, similar to opiates, those with numerous metabolites that themselves can be parent drugs. For example, temazepam and oxazepam in the adjacent chart.
Contrasted to diazepam and its metabolites, clonazepam and lorazepam have their own breakdown pathway and so these tend to be simpler to interpret on LC-MS
Miscellaneous:
A common scenario, even after doing this for many years, is that a metabolite shows up on LC-MS that you have never seen before and doesn’t seem to resemble any drug you’re familiar with. See case 4b below for an example of how you might navigate through this scenario.
FALSE NEGATIVES
False negatives can occur on both IA and LC-MS. There are several explanations for false negatives: 5,27
- Dilute urine (excess fluid intake, diuretic use, pediatric sample)
- Infrequent drug use
- Prolonged time since last use (detection windows vary greatly between drugs, and significant variability even within the same drug)
- Recent ingestion
- Insufficient quantity ingested
- Metabolic factors
- Inappropriate test used
- Elevated urine lactate
- Tampering

For quick UDT interpretation from your smartphone, we would highly recommend our free app “UrInterpret”. In addition to there being sections describing both HARMS and START-IT, there is a section with Cases where you can practice with realistic, common scenarios. The section that we use the most ourselves is called “Quick UDT”. It is a user-friendly way of getting quick answers to your UDT interpretation questions, such as,
For IA,
- The morphine panel is positive, what drugs may have caused this? Or conversely…
- My patient is prescribed hydromorphone, which panels would I expect to be positive?
For LC-MS,
- LC-MS detected hydromorphone, which drugs may have caused this? Or conversely…
- My patient is prescribed morphine, what metabolites may I see on LC-MS?
Visit our website www.harmsprogram.ca/urinterpret to see more about how it works.

